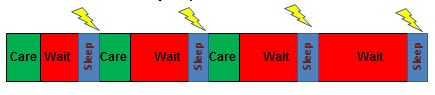
As a definition, 7 days length of stay or longer and over 75 years is the favoured metric. A proportion of these people will have true catastrophic illness and will need to be an inpatient that long. However, a significant proportion have got to that length of stay because of unnecessary waits in the system, the majority of which are internal such as waiting for a decision, a diagnostic test, an intervention, a referral and so on.
An increasing number of health-care providers are measuring, investigating and reporting these delays. This process, with weekly challenge to and by clinical teams, works to drive down the internal delays (waiting for things to happen) that every patient is exposed to. A colleague and clinical advisor to the AFN (acute frailty network), Dr Ian Sturgess, describes this: “Whenever I get teams to peer review long LOS inpatients, I get them to ask 2 questions:
1. What is being done now to get them discharged - the obvious question.
2. What could and should have been done on days 0, 1, 2 etc to prevent them becoming stranded.
"This is the crucial 'learning' and is what an assertive acute frailty service is designed to deliver”

Unable to access - there are another group of patients I worry about who might also be called stranded. That is those with frailty who don’t make it into specific frailty wards / departments. In my clinical time on the acute medicine unit (AMU) I see few, but none-the-less some, patients who don’t get on to the excellent acute frailty unit (AFU) next door because it is full. Does this matter? Well, the AFU is mature and has clear processes to ensure high quality care. CGA is explicit and understood. It is delivered by an energetic and focused team and is normal care.
Patients are dressed and out of bed. There are specialist care givers who understand how to safely transfer the care of people with, or recovering from, frailty. There are even activity leaders. Frail older people in crisis who come to the AMU get a more traditional type of care. It is good, and the AMU has two brilliant discharge facilitators along with visiting therapists. The medical and nursing staffing is as you would expect. I just know which team I would choose to care for me if I were frail.
I’m not advocating a split take, merely recognising a gap. What would it take to get every frail patient to the frailty team first time? And what do we need to do on our AMU to ensure the difference in service provided is insignificant? After all, frailty is everyone’s business. Which leads me neatly into a question.
Have you measured the demand? Are you working to match the capacity? Remembering that capacity is not beds. It is decision makers.
Dr Jack Hawkins - NHS Emergency Care Improvement Programme (ECIP), Clinical Director @jackhawski
