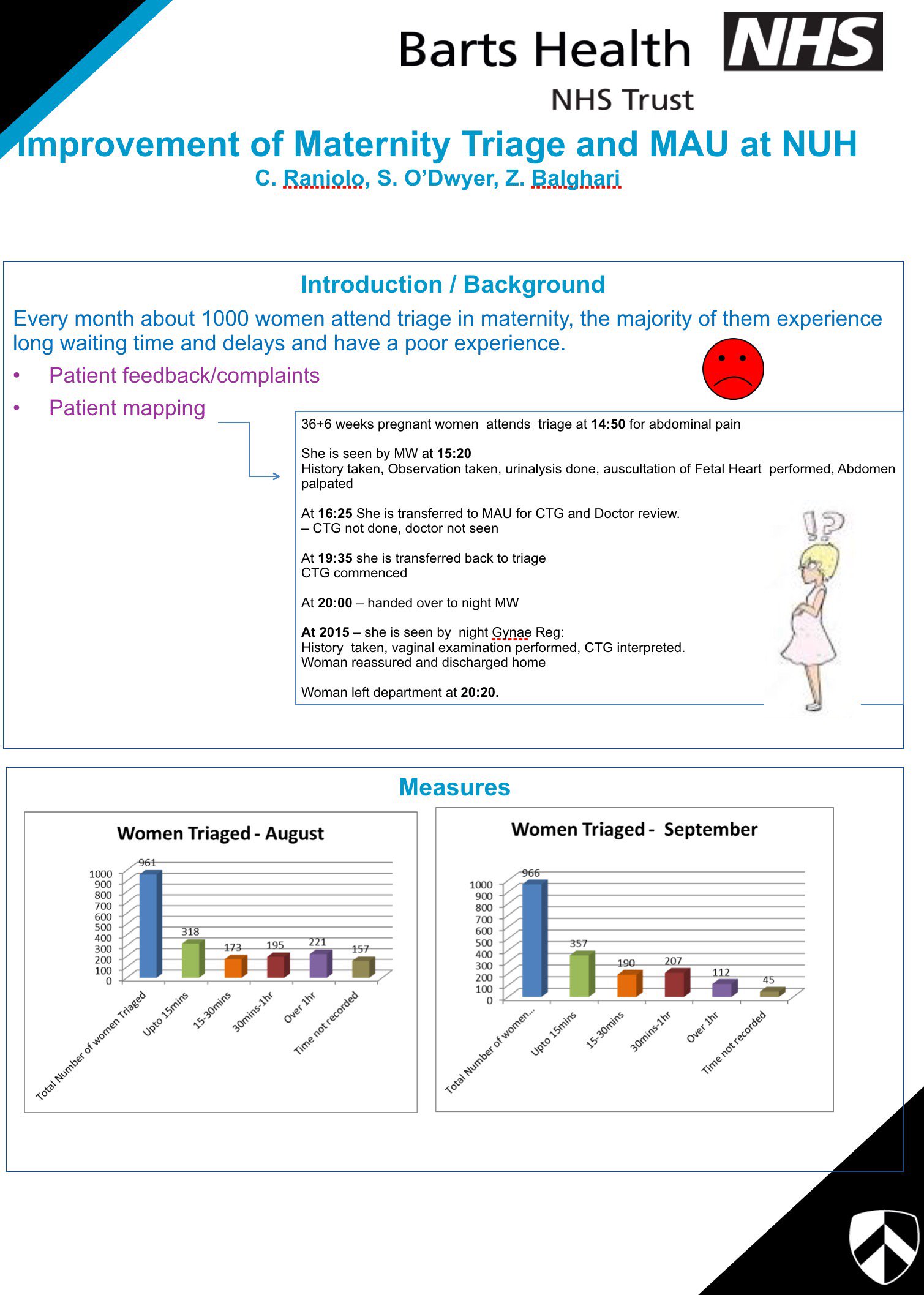
It is a place that sees >1000 pregnant women per month. It is a place where women can walk in with a headache, and turn out to have raging pre-eclampsia. It is a place where women in labour arrive, screaming in pain. It is a place where high-risk women with underlying medical problems come for monitoring and blood tests.
Mostly, it is a place of reassurance – where worried women can see health professionals and be told that their symptoms are not serious. At times, it is a place of crisis – where pregnant women with babies that haven’t moved get told that their babies have passed away, or where a woman with bleeding has to be moved to the operation suite immediately for a Caesarean.
Maternity Triage and Day Assessment is essentially an Emergency Department and a Medical Day Unit, but for pregnant women. It helps women access specialist emergency care without going via the Emergency Department and helps us monitor high-risk women, who otherwise might have been admitted as in-patients.
However, we know from patient complaints and patient mapping that waiting times are often excessively long in the unit. One patient journey took us through a woman who arrived at 2pm with abdominal pain, and did not leave the department until 9pm that night. This breaches the standard of care expected of a general Emergency Department.
We conducted patient and staff surveys, which reveal that although patients are very appreciative of hardworking staff in the unit, the general feeling is that the unit is very pressured. Staff often feel like they are not well supported by the wider team. For example, many staff pointed out that they would regularly be asked to care for a labouring woman in triage because there were not enough staff or beds on the labour ward. This would compromise the care of the individual woman, as well as divert triage staff’s attention away from other women.
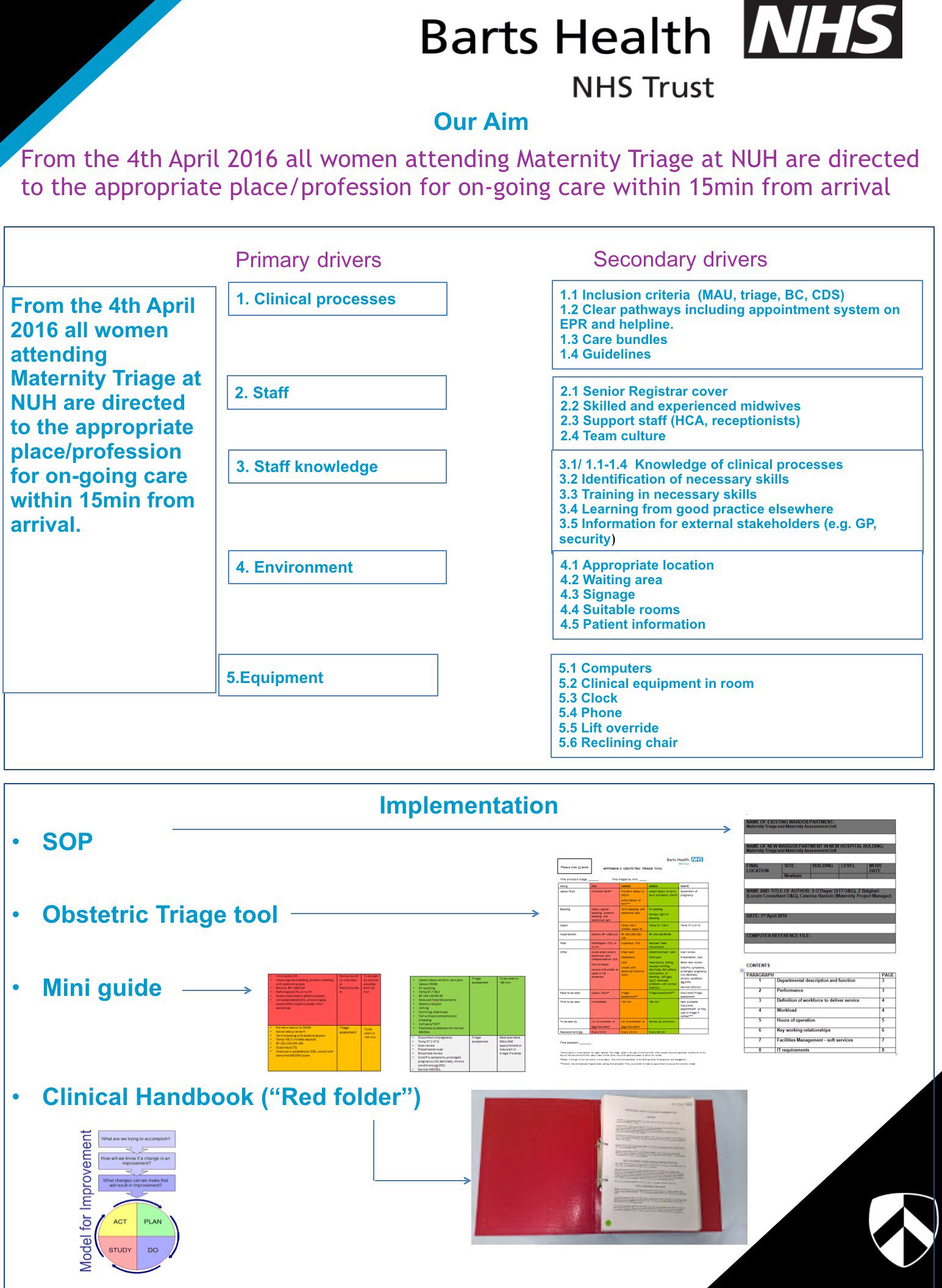
We conducted workshops to determine what the underlying problems and root causes were, and conducted opinion polls on a proposed new way of working. We identified 5 primary drivers which were process, staffing, knowledge, environment and equipment each with multiple secondary drivers.
We are implementing:
• Triage acuity tool
• Assessment Unit appointments system
• Clinical handbook with use of validated care bundles to streamline and standardise care.
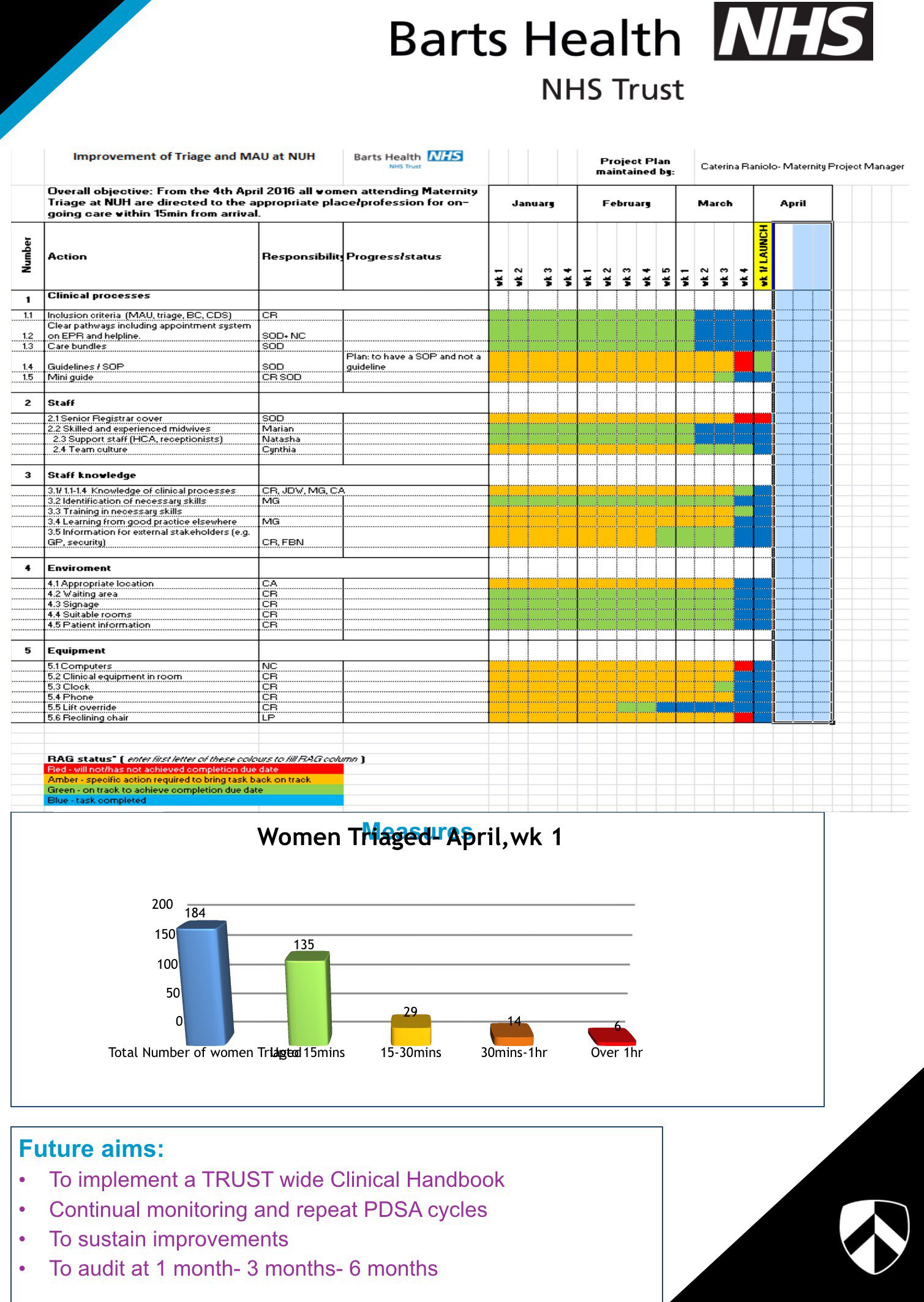
Ongoing audit will be carried out, with key performance indicators being the time taken from arrival to rapid triage (our target is <15 minute), time taken to transfer the woman out of the unit once the decision had been made to admit, and total time spent in the unit (our target is 4h).
[email protected]