
What was the problem?
The driver for implementing criteria-led discharge (CLD) was to improve flow by facilitating weekend discharges.
The team were already practising this informally during the week as patients planned to go home that day were NOT seen on that day’s ward round.
What was the solution?
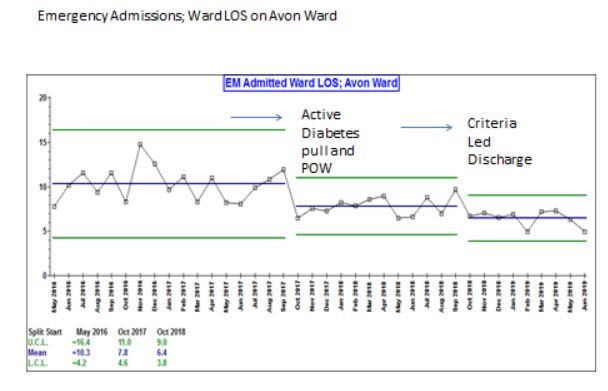
The team had established a robust process for a daily board round with a multi-disciplinary team. They worked with the site management team in bringing the right patients to their ward – ‘Right specialist team first time’. The consultants and the diabetic specialist nurses developed an active pull system whereby patients benefiting from their specialist input who were on other wards were ‘pulled’ to their ward. Departmental annualised job planning was introduced which was transparent and fair. A Consultant Of the Week (COW) model was implemented within the job plan to provide continuity of care.
Once the decision to formally try CLD was taken, the entire team took part in the journey from the beginning. The consultants, nurses, and managers discussed it and created a vision of why, what and the how. This vision was shared and discussed with the rest of the team and the process was co-produced. The process had a start date and was tweaked and perfected with time.
The salient features of this team which made any change easy to embed are the culture they developed:
- There is a flattened hierarchy within the team.
- Respectful challenge is the norm and encouraged.
- Every member of the team has jobs allocated which they take responsibility for and jobs are allocated fairly.
- No member of the team leaves until all the jobs are completed. If you finish your work you help others.
Other enablers which helped weekend discharge:
- Out Patient Antibiotic Therapy (OPAT) services.
- Ambulatory care taking over the continued management of some patients.
What were the learning points?
- Start thinking of patients suitable for CLD on the Thursday board round (All the team agree, challenge and are aware).
- Firm up the list on the Thursday ward round.
- Make sure this is communicated to the patient and family on Thursday.
- TTOs done for those patients between Thursday afternoon and Friday morning (tasks allocated).
- Check again at the Friday board round.
- Friday afternoon – CLD stickers with clear criteria put on patient notes – Nurse discharge or Medical discharge (complexity of the patient decided whether it was the nurse or doctor, and was allocated only after discussion and acceptance from the team). The stickers have been modified with time by the team.
- Monday morning – review list to check if any patients were not discharged and why – Education and feedback to the team.
What were the challenges?
- Junior doctors felt it was more work: The consultants agreed that since it was a new process, they would support them until it was business as usual. So they supported the juniors in ‘exception reporting’ to the educational supervisor if they had to stay back. Once the juniors saw the value to the patients and the support they got, they stopped the reporting. They also learned to incorporate the process into their day time tasks.
- Friday handovers: There is a routine ward handover from the COW of the current week to the COW of the following week on a Friday. The CLD list was initially part of this handover. This long handover kept the juniors from doing the tasks. So the handover was split and the juniors were asked to attend only the CLD handover so the TTOs could be done in a timely way.
- Finding justifications to delay discharge as the criteria missed slightly – Monday morning review of the CLD list to educate and empower nurses and doctors to deviate safely from the criteria, or escalate if necessary, was introduced.
- Long list for out of hours tasks generated by the junior doctors: The consultants took responsibility to challenge the work list for the weekend teams. The list was minimised by removing unnecessary reviews, blood tests etc. which did not change management. The out of hours work from the ward was monitored closely.
What were the results?
The length of stay on the ward fell from 10.3 to 6.4 days.
Next steps and sustainability:
- Roll out to the rest of the wards in the hospital.
- Avon Ward team present their case study at a divisional meeting.
- Care of the Elderly team and other teams keen to follow the example.
- Dr. Mahto invited to the CoE departmental meeting for discussion.
- Slow but steady spread of culture and practice.
- Continue to learn, and make improvements on base ward.
- Recognition of the team’s work at Board level.
Contact:
Dr Rajni Mahto (Consultant in Diabetes and Endocrinology) - [email protected]
Rachel Williams (Associate Director of Operations) - [email protected] @rawbubbles
Dr Jyothi Nippani (Clinical Lead) - @jyothinippani
https://ecist.home.blog/2019/09/04/criteria-led-discharge-cld/
https://improvement.nhs.uk/resources/criteria-led-discharge/