The challenge is then to ensure that AEC services are configured to be available for as many suitable patients as possible. AEC should only be a consideration for patients that previously would have been admitted. The key to this is to systematically use the 6As of managing medical emergency admissions and to monitor the effectiveness of existing AEC.
Understanding whether your AEC service is meeting the true demand (patients that need and receive AEC) and not acting as a supply side driver (attracting additional non-emergency activity) is key to planning future service development. To understand the potential for AEC you will need to undertake some analysis, the approach is described below;
- Undertake a retrospective case note analysis. This could be a continuous period of time e.g. 1 week or selected days. It should include a mix of weekdays & weekends, a minimum of 50 case notes are needed.
- Identify all adult patients referred for emergency admission during the defined periods of time.
- Review each case with an experienced senior clinician. Each case should be judged on its clinical merits alone. The judgement should be whether the patients clinical condition is appropriate for AEC; time of presentation, staffing levels, access to diagnostics etc. should not be a consideration as to whether or not a patient should be categorised as suitable for AEC. This will be addressed later.
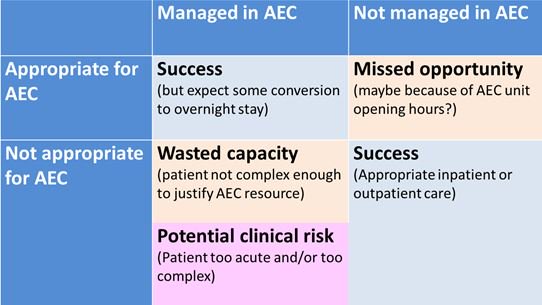
- Not managed in AEC & Not appropriate for AEC – this group of patients have been appropriately managed as in-patients
- Managed in AEC & Appropriate for AEC selection – this is the group that have been successfully identified and managed in AEC
- Not managed in AEC & appropriate for AEC selection – this is the opportunity for AEC development, these are ‘missed patients’.
- Managed in AEC & not appropriate for AEC – this could be either non-urgent cases which is wasted capacity or patients that have been sent to AEC waiting for admission which may constitute a clinical risk.
For group 3, we need to understand why patients were not managed in AEC. There are a range of reasons why this may have been the case, some of which are highlighted below.
- AEC services not available due to opening hours, staffing
- No access to diagnostics
- Conservative clinical judgement
- Lack of awareness of services
- Lack of capacity
- Lack of clinical experience
- AEC is shut e.g. out of hours
- Inexperienced decision makers
- Poor understanding of AEC services
- Emergency pressures
- Used inappropriately for elective cases (any elective cases should be scheduled pre 11am)
- Patient sicker than expected
- Alternative diagnosis established
- Identified as needing treatment only available to in-patients
- Patients admitted to meet targets
The data can be presented in tabulated form using the grid below.
Analysis of the group 3 missed opportunities will identify the specific steps required to take the service forward. This could include agreeing a process for out of hours referrals, extending opening hours in the evening and weekends, improved training for staff handling referrals or ensuring access to key diagnostic services are available.
Analysis of group 4 should be used to identify if the selection process for AEC is operating effectively. The results can be fed back to the team with modifications to the streaming process as necessary.
The analysis should be repeated to check on progress, in particular, whether the service changes have been successfully embedded in clinical practice.
For more information on maximising AEC go to http://www.ambulatoryemergencycare.org.uk
Author - Dr Vincent Connolly - Consultant Physician (The James Cook University Hospital) & Medical Director Emergency Care Improvement Programme
You can follow Vincent on Twitter @vincentconnolly