Our processes for unscheduled care are unequal and inefficient. Patients expected from GP referrals can wait unnecessarily long for a specialty team to clerk, while patients coming by ambulance are seen promptly by ED (emergency department) doctors. Junior doctors re-clerk patients, which adds in a delay to the senior-decision making process and often no added value – someone who was the ED F2 1 month ago is now the clerking medical F2.
Our performance data from the second half of 2015 indicated huge room for improvement: the average time for patients to get a decision to admit (DTA) was 5 hours, with approximately 30% of patients getting a DTA within 3hour and 45 minutes – a time that is crucial for moving patients out of A&E within 4 hours.
What is single clerking?
The single clerking model is a change in culture: it brings together all the specialty on-call doctors with ED doctors as one acute floor team, with the ultimate goal to deliver efficient and excellent care, every time. Essentially, it ensures that patients are treated equally, regardless of the mode of presentation and get to a senior decision maker at the earliest opportunity.
Aims
- Stop duplication of work: patients receive one full clerking only
- Consolidate paperwork: 5+ clerking proformas reduced into one form for all, with all medications on a drug chart (previously 3+ places to prescribe)
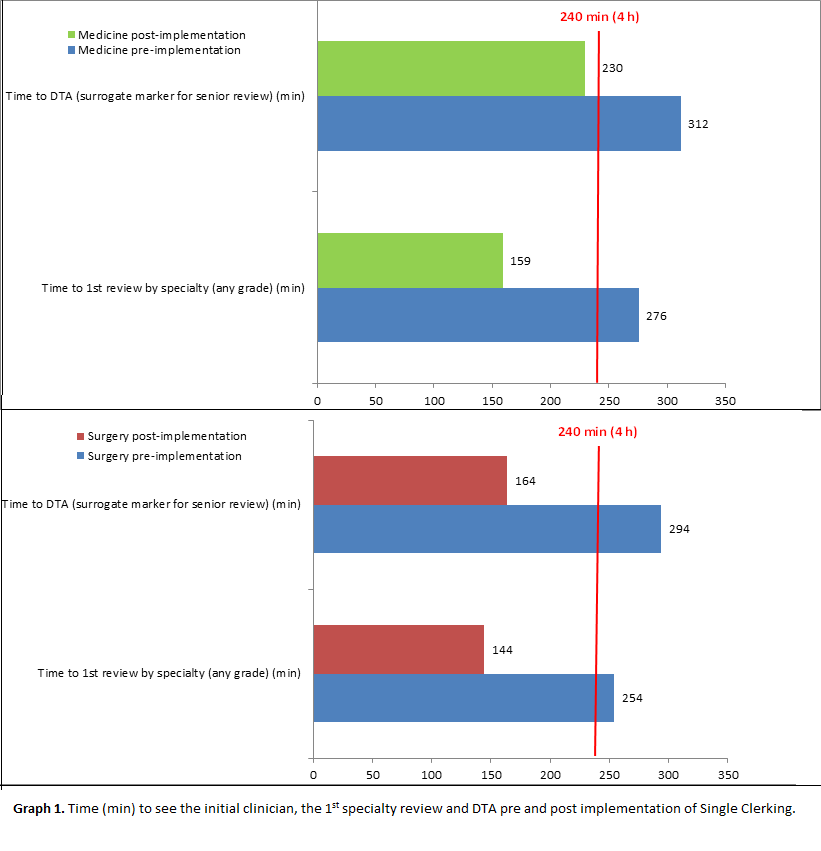
- Reduce the time patients wait for a senior clinical review: direct from clerking doctor to senior decision maker
- Free juniors for more educational opportunities: clerking juniors assess undifferentiated patients, review their patients with relevant senior and specialty juniors have more time to engage in training opportunities such as theatre and procedures
- The acute floor ethos: working together as one team rather than in individual silos, to encourage collaborative decision making. Doctors, nurses, outreach and site managers meet as one acute floor on a daily basis
Challenges
- Changing culture: single clerking is a change to working practices for many doctors and nurses
- Moving to one acute floor team: varying shift patterns and handover times
- The proforma: creating one document that suits all specialties
- Defining responsibilities: acute consultants now have many more juniors clerking their patients – clear processes are needed to ensure completion of tasks and safe handover