Emergency admission to hospital is a major event in people’s lives. It should never happen because it is easy to admit or to access services that could be available as an out-patient or to administer treatment that may be available closer to home or to get a specialist opinion. All of these are spurious reasons for an emergency admission. To transform emergency healthcare we need to understand why we put patients through this process when alternatives exist and operate effectively across the country but haven’t been widely implemented.
Emergency admission implies a patient is sick requiring a high level of intervention, as such all proposed emergency admissions should prompt a clinical conversation between senior doctors, ideally consultants.
The clinical conversation should occur at the point of referral. The person requesting admission from ED, primary care or elsewhere, should be able to have immediate access to the specialist team to discuss the patient. The discussion should include
- Clinical Situation, the EWS, presenting symptoms, related clinical issues
- Background, clinical history, social circumstances • Clinical assessment, working diagnosis
- Request, a clear indication of why the patient needs admission
- The patient’s preference
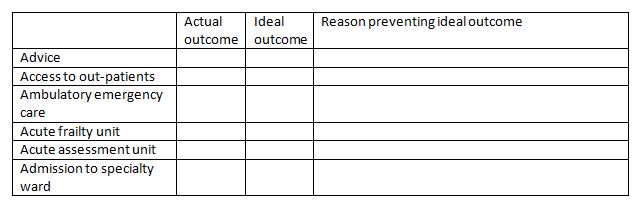
- Advice - following the clinical conversation a suggested clinical management plan that allows the patient to return home, perhaps with follow up in primary care
- Access to out-patient services - patients may require a specialist assessment or ongoing management of a long term condition
- Ambulatory Emergency Care - patients that are clinically stable who require further specialist evaluation, diagnosis or treatment including surgical procedures
- Acute Frailty Unit - to provide comprehensive geriatric assessment for frail older patients
- Acute Assessment Units - to stabilise, monitor & diagnose and manage patients likely to need to admission
- Admission to specialty ward directly - for agreed clinical pathways, specialised clinical presentations, need for critical care support
Implementation and monitoring the 6
As Many systems will have elements of the 6 As in place but are they available in a comprehensive and systematic way? It is important to understand how the clinical decision making process and the availability of services is aligned. This should be monitored on a regular basis and used to inform future service developments. A senior doctor or improvement manager should be assigned to work on site with the ED team and the point of primary care referral. Each request for admission should be monitored to understand why admission has been requested and whether an alternative could have been offered in ideal circumstances ie not constrained by current service provision. The data should be recorded in the chart below to help understand the opportunities for service improvement.
At the end of the period of data collection the most common reasons should be identified, many of these may be resolvable by the clinical team. Those that cannot should be escalated to the responsible executive for action.
Dr Vincent Connolly - Consultant Physician (The James Cook University Hospital) & Medical Director NHS Emergency Care Improvement Programme (ECIP)